
ATLL
What is ATLL?
Adult T cell leukaemia/lymphoma (ATLL) is a rare blood cancer seen only in people infected with HTLV-1.
HTLV-1 infection is maintained in the body because it can integrate its own viral DNA into the host DNA. It mostly incorporates itself into a specific type of immune cell, the CD4+ T-lymphocyte. We can measure this using PCR by sampling and testing the cells in the blood.
In patients with ATLL, these infected HTLV + /CD4+ T-lymphocyte multiply uncontrollably. This can occur in the bone marrow, blood stream, lymph nodes and skin. ATLL cells replace healthy tissue and prevent healthy tissue from functioning normally. ATLL can progress very slowly or very fast. This is why there are four subtypes of ATLL.
Adult T cell leukaemia/lymphoma (ATLL) is a rare blood cancer seen only in people infected with HTLV-1.
HTLV-1 infection is maintained in the body because it can integrate its own viral DNA into the host DNA. It mostly incorporates itself into a specific type of immune cell, the CD4+ T-lymphocyte. We can measure this using PCR by sampling and testing the cells in the blood.
In patients with ATLL, these infected HTLV + /CD4+ T-lymphocyte multiply uncontrollably. This can occur in the bone marrow, blood stream, lymph nodes and skin. ATLL cells replace healthy tissue and prevent healthy tissue from functioning normally. ATLL can progress very slowly or very fast. This is why there are four subtypes of ATLL.

Who gets ATLL?
Luckily only 3 to 5 out of 100 people infected with HTLV-1 ever develop ATLL. Only persons infected with HTLV-1 get ATLL.
Japanese HTLV-1 carriers seem to have the highest risk of developing ATLL.
The interval between HTLV-1 infection and the onset of ATLL is often more than 40 years. In the UK, the average age of first presentation of a patient with ATLL is 50 years. The HTLV proviral load is > 5% in most ATLL types.
No trigger has been identified that is known to initiate ATLL and so far no method has been identified that can prevent ATLL from developing.
Luckily only 3 to 5 out of 100 people infected with HTLV-1 ever develop ATLL. Only persons infected with HTLV-1 get ATLL.
Japanese HTLV-1 carriers seem to have the highest risk of developing ATLL.
The interval between HTLV-1 infection and the onset of ATLL is often more than 40 years. In the UK, the average age of first presentation of a patient with ATLL is 50 years. The HTLV proviral load is > 5% in most ATLL types.
No trigger has been identified that is known to initiate ATLL and so far no method has been identified that can prevent ATLL from developing.
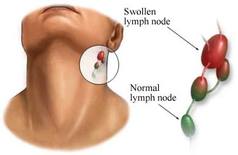
 Swollen lumps found in the neck
Swollen lumps found in the neck
What are ATLL subtypes?
The ATLL sub-classification is called the Shimoyama ATLL classification. The subtypes are:
ATLL can affect the blood, which is called the acute leukaemic form. In this case there are too many HTLV+ /CD4+ T-lymphocytes in the blood. Lymphnodes are also affected.
Lymphnodes are parts of the body where healthy immune cells are produced. The patient feels enlarged lumps in the neck or under the armpits. These can be painful or painless. Most people have one or two small lumps but in the case of ATLL these lumps are pretty large. Since the blood stream is not affected one or two of these lumps need to be removed and tested to be sure of diagnosis. This is called a biopsy.
ATLL can affect only the lymphnodes, which is called ATLL lymphoma. The blood is not affected.
These two subtypes are thought to be aggressive since people who develop it become ill very quickly. The other two subtypes are called chronic and smoldering. Both are diagnosed mainly through specific blood tests: lymphocyte count, HTLV proviral load, LDH and calcium levels. These two types progress much slower and are less aggressive cancers.
ATLL cells can also grow in the skin, this is called cutaneous ATLL.
The ATLL sub-classification is called the Shimoyama ATLL classification. The subtypes are:
- Leukaemic ATLL
- Lymphomatous ATLL
- Chronic ATLL
- Smoldering ATLL
ATLL can affect the blood, which is called the acute leukaemic form. In this case there are too many HTLV+ /CD4+ T-lymphocytes in the blood. Lymphnodes are also affected.
Lymphnodes are parts of the body where healthy immune cells are produced. The patient feels enlarged lumps in the neck or under the armpits. These can be painful or painless. Most people have one or two small lumps but in the case of ATLL these lumps are pretty large. Since the blood stream is not affected one or two of these lumps need to be removed and tested to be sure of diagnosis. This is called a biopsy.
ATLL can affect only the lymphnodes, which is called ATLL lymphoma. The blood is not affected.
These two subtypes are thought to be aggressive since people who develop it become ill very quickly. The other two subtypes are called chronic and smoldering. Both are diagnosed mainly through specific blood tests: lymphocyte count, HTLV proviral load, LDH and calcium levels. These two types progress much slower and are less aggressive cancers.
ATLL cells can also grow in the skin, this is called cutaneous ATLL.
 'Flower' cells, as seen under a microscope
'Flower' cells, as seen under a microscope
What is the natural history of the different types of ATLL?
Acute ATLL Usually patients develop problems rapidly, and quite quickly ATLL becomes life threatening if not treated. Common problems are: skin rash, many large lumps found on the neck, armpits, groin and frequent infections. Patients are tired, have night sweats and lose weight. These are called B symptoms. Examinations may reveal enlargement of the liver and spleen. Blood tests show a raised white blood count, typical abnormal ATLL cells, called flower celled and high levels of calcium and LDH in the blood. X-rays may show bone damage.
Lymphomatous ATLL Is characterised by many large lumps, called lymph nodes anywhere in the body, for example, the neck, axilla, groin, stomach. Patients are often tired, have night sweats and lose weight. These are called B symptoms. The blood count is often completely normal and very few or no flower cells are found in the blood. For some reason almost all the cancerous lymphocytes stay in the lymph nodes.
Chronic ATLL The common symptoms are a skin rash and B symptoms but the condition is detected on routine blood tests. Lymph nodes, liver or spleen may be enlarged. This ATLL type gets worse much more slowly, than the acute or lymphoma ATLL. The white cell count may be raised and abnormal T-cells are seen in the blood but the calcium level in the blood is normal.
Smoldering ATLL The disease is present in a very mild form and may be found on routine blood tests only showing flower cells in the blood but normal cell counts. There may be some skin lesions but lymph nodes, spleen and liver are normal.
Acute ATLL Usually patients develop problems rapidly, and quite quickly ATLL becomes life threatening if not treated. Common problems are: skin rash, many large lumps found on the neck, armpits, groin and frequent infections. Patients are tired, have night sweats and lose weight. These are called B symptoms. Examinations may reveal enlargement of the liver and spleen. Blood tests show a raised white blood count, typical abnormal ATLL cells, called flower celled and high levels of calcium and LDH in the blood. X-rays may show bone damage.
Lymphomatous ATLL Is characterised by many large lumps, called lymph nodes anywhere in the body, for example, the neck, axilla, groin, stomach. Patients are often tired, have night sweats and lose weight. These are called B symptoms. The blood count is often completely normal and very few or no flower cells are found in the blood. For some reason almost all the cancerous lymphocytes stay in the lymph nodes.
Chronic ATLL The common symptoms are a skin rash and B symptoms but the condition is detected on routine blood tests. Lymph nodes, liver or spleen may be enlarged. This ATLL type gets worse much more slowly, than the acute or lymphoma ATLL. The white cell count may be raised and abnormal T-cells are seen in the blood but the calcium level in the blood is normal.
Smoldering ATLL The disease is present in a very mild form and may be found on routine blood tests only showing flower cells in the blood but normal cell counts. There may be some skin lesions but lymph nodes, spleen and liver are normal.

What problems do ATLL patients notice?
The reported problems depend on which type of ATLL the patient has developed. The most common are: the B symptoms (tiredness, weight loss, night sweats) as well as skin rashes, appearance of lumps in the areas like neck, armpits, groin, sometimes stomach ache, fever and thirst.
How is ATLL diagnosed?
Usually the patient will present with one or more of the problems above which will suggest the diagnosis of a leukaemia or lymphoma. The doctor needs to diagnose a T cell cancer and then HTLV before ATLL can be confirmed.
Your doctor will arrange for many tests such as:
The reported problems depend on which type of ATLL the patient has developed. The most common are: the B symptoms (tiredness, weight loss, night sweats) as well as skin rashes, appearance of lumps in the areas like neck, armpits, groin, sometimes stomach ache, fever and thirst.
How is ATLL diagnosed?
Usually the patient will present with one or more of the problems above which will suggest the diagnosis of a leukaemia or lymphoma. The doctor needs to diagnose a T cell cancer and then HTLV before ATLL can be confirmed.
Your doctor will arrange for many tests such as:
- Blood tests
- HTLV-1 antibodies
- HTLV-1 proviral load
- T cell subset (CD4/CD25/DR)
- T cell clonality
- Lymphnode, bone marrow and/or skin biopsy
- CT scan of chest and abdomen to look for enlarged lymph nodes, liver and spleen
- Lumbar puncture to look for evidence of spread to the brain